Levonorgestrel
 | |
 | |
| Clinical data | |
|---|---|
| Trade names | Plan B, others |
| AHFS/Drugs.com | Monograph |
| MedlinePlus | a610021 |
| Pregnancy category |
|
| Routes of administration | Implant, insert (extended-release), by mouth |
| ATC code | G03AC03 (WHO) G03AD01 (WHO) |
| Legal status | |
| Legal status |
|
| Pharmacokinetic data | |
| Bioavailability | ~100% |
| Protein binding | 55% |
| Metabolism | Liver via CYP3A4 |
| Biological half-life | 36 ± 13 hours |
| Excretion | Kidney: 45%; Feces:32% |
| Identifiers | |
| |
| CAS Number |
797-63-7 |
| PubChem (CID) | 13109 |
| IUPHAR/BPS | 2881 |
| DrugBank |
DB00367 |
| ChemSpider |
12560 |
| UNII |
5W7SIA7YZW |
| KEGG |
D00950 |
| ChEBI |
CHEBI:6443 |
| ChEMBL |
CHEMBL1389 |
| Chemical and physical data | |
| Formula | C21H28O2 |
| Molar mass | 312.446 g/mol |
| 3D model (Jmol) | Interactive image |
| |
| |
| (verify) | |
Levonorgestrel is a manufactured hormone used in a number of birth control methods.[1] In pill form, sold under the brand name Plan B among others, it is useful within 120 hours as emergency birth control. It becomes less effective the longer after sex and only works before pregnancy has occurred.[1] It is also combined with an estrogen to make combined oral birth control pill.[2] Within an IUD, sold as Mirena among others, it is effective for long term prevention of pregnancy.[1] An implantable form of levonorgestrel is also available in some countries.[3]
Common side effects include nausea, breast tenderness, headaches, and increased, decreased, or irregular menstrual bleeding. When used as a form of emergency contraception, if pregnancy occurs, there is no evidence its use harms the baby. It is safe to use during breastfeeding. Birth control that contains levonorgestrel will not change the risk of sexually transmitted infections. It works mostly by decreasing ovulation and closing off the cervix to prevent the passage of sperm.[1]
Levonorgestrel was first made in the 1960s and its use as a method of birth control began in the 1980s.[4] It is on the World Health Organization's List of Essential Medicines, the most important medication needed in a basic health system.[5] It is available as a generic medication.[6] The wholesale cost in the developing world costs between 0.23 and 1.65 USD for the dose required for emergency birth control.[7] In the United States it is over the counter for all ages.[8]
Medical uses
Oral birth control
At low doses, levonorgestrel is used in monophasic and triphasic formulations of combined oral contraceptive pills, with available monophasic doses ranging from 100-250 µg, and triphasic doses of 50 µg/75 µg/125 µg.
At very low daily dose of 30 µg, levonorgestrel is used in some progestogen only pill formulations.
Emergency birth control
Levonorgestrel is used in emergency contraceptive pills (ECPs), both in a combined Yuzpe regimen which includes estrogen, and as a levonorgestrel-only method. The levonorgestrel-only method uses levonorgestrel 1.5 mg (as a single dose or as two 0.75 mg doses 12 hours apart) taken within 3 days of unprotected sex, with one study indicating that beginning as late as 120 hours (5 days) after intercourse could be effective.
The primary mechanism of action of levonorgestrel as a progestogen-only emergency contraceptive pill is, according to International Federation of Gynecology and Obstetrics (FIGO), to prevent fertilization by inhibition of ovulation and thickening of the mucosa of cervix.[9][10][11][12] FIGO has stated that: "review of the evidence suggests that LNG [levonorgestreol] ECPs cannot prevent implantation of a fertilized egg. Language on implantation should not be included in LNG ECP product labeling."[13][14] In November 2013, the European Medicines Agency (EMA) approved a change to the label saying it cannot prevent implantation of a fertilized egg.[15]
Other studies still find the evidence to be unclear.[16] While it is unlikely that emergency contraception affects implantation it is impossible to completely exclude the possibility of post-fertilization effect.[17]
In November 2013, the EMA also approved a change to the label for HRA Pharma's NorLevo saying: "In clinical trials, contraceptive efficacy was reduced in women weighing 75 kg [165 pounds] or more, and levonorgestrel was not effective in women who weighed more than 80 kg [176 pounds]."[15][18][19] In November 2013 and January 2014, the FDA and the EMA said they were reviewing whether increased weight and body mass index (BMI) reduce the efficacy of emergency contraceptives.[15]
Intrauterine device
Levonorgestrel is the active ingredient in the Mirena & Skyla (Jaydess) intrauterine system.
Contraceptive implants
Levonorgestrel is the active ingredient in Norplant and Jadelle.
Hormone replacement therapy
Levonorgestrel is combined with 17-beta estradiol in the estrogen patch.
Side effects
After intake of levonorgestrel 1.5 mg in clinical trials, very common effects (reported by 10% or more) included: dizziness, headache, nausea, abdominal pain, uterine pain, delay of menstruation, heavy menstruation, uterine bleeding, or fatigue; common effects (reported by 1% to 10%) included diarrhea, vomiting, or painful menstruation; these effects usually disappeared within 48 hours.[20]
Chemistry
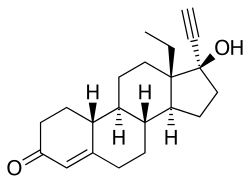
Levonorgestrel is an estrane steroid derived from testosterone and is also known as 17α-ethynyl-18-methyl-19-nortestosterone or as 17α-ethynyl-18-methylestr-4-en-17β-ol-3-one. Levonorgestrel (levo=left) is one form of a steroid, norgestrel, that exists in two mirror image left and right forms (see Chirality (chemistry)). It is the hormonally active levorotatory enantiomer of the racemic mixture. It is a gonane progestin derived from 19-nortestosterone.[21]
Its in vitro relative binding affinities at human steroid hormone receptors are: 323% that of progesterone at the progesterone receptor, 58% that of testosterone at the androgen receptor, 17% that of aldosterone at the mineralocorticoid receptor, 7.5% that of cortisol at the glucocorticoid receptor, and <0.02% that of estradiol at the estrogen receptor.[22]
If taken together with drugs that induce the CYP3A4 cytochrome liver enzyme, levonorgestrel may be metabolized faster and may have lower efficacy.
History
Levonorgestrel was first introduced in 1968, as an oral contraceptive in combination with ethinyl estradiol.[23]
Society and culture
Names
Levonorgestrel is also chemically known as l-norgestrel and D-norgestrel. It is often referred to as the "morning after pill".
There are many brand names for levonorgestrel-only ECPs, including: Nogestat, AfterPill, Escapelle, Plan B, Levonelle, Glanique, NorLevo, Postinor-2, i-pill, Next Choice, 72-HOURS.[24]
Over-the-counter
In 2013 the FDA approved Plan B One-Step to be sold without a prescription to women of all ages.[25]
Indian Health Services
A policy update in 2015 required all Indian Health Services-run pharmacies, clinics, and emergency departments to have Plan B One-Step in stock, to distribute it to any woman (or her representative) who asked for it without a prescription, age verification, registration or any other requirement, to provide orientation training to all staff regarding the medication, to provide unbiased and medically accurate information about emergency contraception, and to make someone available at all times to distribute the pill in case the primary staffer objected to providing it on religious or moral grounds.[26]
References
- 1 2 3 4 "Progestins (Etonogestrel, Levonorgestrel, Norethindrone)". The American Society of Health-System Pharmacists. Retrieved Aug 21, 2015.
- ↑ Postgraduate Gynecology. Jaypee Brothers Medical Pub. 2011. p. 159. ISBN 9789350250822.
- ↑ "Chapter 1". Research on reproductive health at WHO : biennial report 2000-2001. Geneva: World health organization. 2002. ISBN 9789241562089.
- ↑ Science and Political Controversy. Santa Barbara: ABC-CLIO. 2014. p. 97. ISBN 9781610693202.
- ↑ "WHO Model List of EssentialMedicines" (PDF). World Health Organization. October 2013. Retrieved 22 April 2014.
- ↑ Hamilton, Richard J. (2014). Tarascon pocket pharmacopoeia : 2014 deluxe lab-pocket edition (15th ed.). Sudbury: Jones & Bartlett Learning. pp. 310–312. ISBN 9781284053999.
- ↑ "Levonorgestrel". International Drug Price Indicator Guide. Retrieved 21 August 2015.
- ↑ "FDA approves Plan B One-Step emergency contraceptive for use without a prescription for all women of child-bearing potential". June 20, 2013. Retrieved 2 February 2016.
- ↑ Trussell, James; Schwarz, Eleanor Bimla (2011). "Emergency contraception". In Hatcher, Robert A.; Trussell, James; Nelson, Anita L.; Cates, Willard Jr.; Kowal, Deborah; Policar, Michael S. Contraceptive technology (20th revised ed.). New York: Ardent Media. pp. 113–145. ISBN 978-1-59708-004-0. ISSN 0091-9721. OCLC 781956734. p. 121:
Mechanism of action
Copper-releasing IUCs
When used as a regular or emergency method of contraception, copper-releasing IUCs act primarily to prevent fertilization. Emergency insertion of a copper IUC is significantly more effective than the use of ECPs, reducing the risk of pregnancy following unprotected intercourse by more than 99%.2,3 This very high level of effectiveness implies that emergency insertion of a copper IUC must prevent some pregnancies after fertilization.
Emergency contraceptive pills
To make an informed choice, women must know that ECPs—like the birth control pill, patch, ring, shot, and implant,76 and even like breastfeeding77—prevent pregnancy primarily by delaying or inhibiting ovulation and inhibiting fertilization, but may at times inhibit implantation of a fertilized egg in the endometrium. However, women should also be informed that the best available evidence indicates that ECPs prevent pregnancy by mechanisms that do not involve interference with post-fertilization events.
ECPs do not cause abortion78 or harm an established pregnancy. Pregnancy begins with implantation according to medical authorities such as the US FDA, the National Institutes of Health79 and the American College of Obstetricians and Gynecologists (ACOG).80
Ulipristal acetate (UPA). One study has demonstrated that UP can delay ovulation.81... Another study found that UPA altered the endometrium, but whether this change would inhibit implantation is unknown.82
p. 122:
Progestin-only emergency contraceptive pills. Early treatment with ECPs containing only the progestin levonorgestrel has been show to impair the ovulatory process and luteal function.83–87
p. 123:
Combined emergency contraceptive pills. Several clinical studies have shown that combined ECPs containing ethinyl estradiol and levonorgestrel can inhibit or delay ovulation.107–110 - ↑ RCOG Faculty of Sexual; Reproductive Healthcare; Clinical Effectiveness Unit (January 2012). Clinical guidance: emergency contraception (PDF). London: Royal College of Obstetricians and Gynaecologists. ISSN 1755-103X. Retrieved 2012-04-30. p.3:
How does EC work?
In 2002, a judicial review ruled that pregnancy begins at implantation, not fertilisation.8 The possible mechanisms of action should be explained to the patient as some methods may not be acceptable, depending on individual beliefs about the onset of pregnancy and abortion.
Copper-bearing intrauterine device (Cu-IUD). Copper is toxic to the ovum and sperm and thus the copper-bearing intrauterine device (Cu-IUD) is effective immediately after insertion and works primarily by inhibiting fertilisation.9–11 A systematic review on mechanisms of action of IUDs showed that both pre- and postfertilisation effects contribute to efficacy.11 If fertilisation has already occurred, it is accepted that there is an anti-implantation effect,12,13
Levonorgestrel (LNG). The precise mode of action of levonorgestrel (LNG) is incompletely understood but it is thought to work primarily by inhibition of ovulation.16,17
Ulipristal acetate (UPA). UPA’s primary mechanism of action is thought to be inhibition or delay of ovulation.2 - ↑ UNDP/UNFPA/WHO/World Bank Special Programme of Research, Development and Research Training in Human Reproduction (HRP) (March 25, 2010). "Fact sheet on the safety of levonorgestrel-alone emergency contraceptive pills (LNG ECPs)" (PDF). Geneva: World Health Organization.
Can LNG ECPs cause an abortion?
LNG ECPs do not interrupt an established pregnancy or harm a developing embryo.15 The evidence available to date shows that LNG ECP use does not prevent a fertilized egg from attaching to the uterine lining. The primary mechanism of action is to stop or disrupt ovulation; LNG ECP use may also prevent the sperm and egg from meeting.16 - ↑ Speroff, Leon; Darney, Philip D. (2011). "Special uses of oral contraception: emergency contraception, the progestin-only minipill". A clinical guide for contraception (5th ed.). Philadelphia: Lippincott Williams & Wilkins. pp. 153–166. ISBN 978-1-60831-610-6. p. 155:
Emergency postcoital contraception
Levonorgestrel
Mechanism and efficacy - ↑ Belluck, Pam (June 6, 2012). "No abortion role seen for morning-after pill". The New York Times. p. A1.
Belluck, Pam (June 6, 2012). "Drug's nickname may have aided politicization". The New York Times. p. A14. - ↑ International Federation of Gynecology and Obstetrics (FIGO) and International Consortium for Emergency Contraception (ICEC) (April 4, 2011). "Mechanism of action: How do levonorgestrel-only emergency contraceptive pills (LNG ECPs) prevent pregnancy?" (PDF). London: International Federation of Gynecology and Obstetrics.
Levonorgestrel-only emergency contraceptive pills:
• Interfere with the process of ovulation;
• May possibly prevent the sperm and the egg from meeting.
Implications of the research:
• Inhibition or delay of ovulation is LNG ECPs principal and possibly only mechanism of action.
• Review of the evidence suggests that LNG-ECs cannot prevent implantation of a fertilized egg. Language on implantation should not be included in LNG ECP product labeling.
• The fact that LNG-ECs have no demonstrated effect on implantation explains why they are not 100% effective in preventing pregnancy, and are less effective the later they are taken. Women should be given a clear message that LNG-ECs are more effective the sooner they are taken.
• LNG ECPs do not interrupt a pregnancy (by any definition of the beginning of pregnancy). However, LNG ECPs can prevent abortions by reducing unwanted pregnancies. - 1 2 3 Belluck, Pam (November 26, 2013). "New birth control label counters lawsuit claim; European authorities found that a drug like Plan B One-Step cannot prevent fertilized eggs from implanting in the womb". The New York Times. Retrieved March 5, 2014.
HRA Pharma (November 2013). "NorLevo 1.5 mg tablet Patient Information Leaflet (PIL)" (PDF). Dublin: Irish Medicines Board. Retrieved March 5, 2014.NorLevo works by stopping your ovaries from releasing an egg. It cannot stop a fertilized egg from attaching to the womb.
HRA Pharma (November 2013). "NorLevo 1.5 mg tablet Summary of Product Characteristics (SPC)". Dublin: Irish Pharmaceutical Healthcare Association. Retrieved March 5, 2014.|chapter=ignored (help)
European Medicines Agency (January 24, 2014). "Review of emergency contraceptives started". London: European Medicines Agency. Retrieved March 5, 2014. - ↑ Mozzanega, B; Cosmi, E (June 2011). "How do levonorgestrel-only emergency contraceptive pills prevent pregnancy? Some considerations.". Gynecological Endocrinology. 27 (6): 439–42. doi:10.3109/09513590.2010.501885. PMID 20670097.
- ↑ Leung, VW; Levine, M; Soon, JA (February 2010). "Mechanisms of action of hormonal emergency contraceptives.". Pharmacotherapy. 30 (2): 158–68. doi:10.1592/phco.30.2.158. PMID 20099990.
- ↑ Glasier, Anna; Cameron, Sharon T.; Blithe, Diana; Scherrer, Bruno; Mathe, Henri; Levy, Delphine; Gainer, Erin; Ulmann, Andre (October 2011). "Can we identify women at risk of pregnancy despite using emergency contraception? Data from randomized trials of ulipristal acetate and levonorgestrel". Contraception. 84 (4): 363–367. doi:10.1016/j.contraception.2011.02.009. PMID 21920190.
- ↑ Trussell, James; Raymond, Elizabeth G.; Cleland, Kelly (February 2014). "Emergency contraception: a last chance to prevent unintended pregnancy" (PDF). Princeton: Office of Population Research at Princeton University, Association of Reproductive Health Professionals. Retrieved April 9, 2014.
- ↑ HRA Pharma (November 2013). "NorLevo 1.5 mg tablet Summary of Product Characteristics (SPC)". Dublin: Irish Pharmaceutical Healthcare Association. Retrieved April 9, 2014.
|chapter=ignored (help) - ↑ Edgren RA, Stanczyk FZ (1999). "Nomenclature of the gonane progestins". Contraception. 60 (6): 313. doi:10.1016/S0010-7824(99)00101-8. PMID 10715364.
- ↑ Sitruk-Ware R (2006). "New progestagens for contraceptive use". Hum Reprod Update. 12 (2): 169–78. doi:10.1093/humupd/dmi046. PMID 16291771.
- ↑ Archer, David F.; Maheux, Rodolphe; DelConte, Anthony; O’Brien, Francis B. (1999). "Efficacy and safety of a low-dose monophasic combination oral contraceptive containing 100 μg levonorgestrel and 20 μg ethinyl estradiol (Alesse®)". American Journal of Obstetrics and Gynecology. 181 (5): S39–S44. doi:10.1016/S0002-9378(99)70362-5. ISSN 0002-9378.
- ↑ Trussell, James; Cleland, Kelly (2007-04-10). "Emergency Contraceptive Pills Worldwide". Princeton University. Retrieved 2007-05-28.
- ↑ http://www.fda.gov/newsevents/newsroom/pressannouncements/ucm358082.htm
- ↑ Rankin, Kenrya. "This Policy Gives Native Women Equal Access to Emergency Contraception". Colorlines. Retrieved 2015-10-24.
External links
- Levonelle manufacturer's product information from Schering
- Monograph for levonorgestrel - Uk Medicines Information
- U.S. National Library of Medicine: Drug Information Portal - Levonorgestrel