Trigeminal neuralgia
| Trigeminal neuralgia | |
|---|---|
| tic douloureux,[1] prosopalgia,[2] Fothergill's disease[3] suicide disease[4] | |
|
The trigeminal nerve and its three major divisions (shown in yellow): the ophthalmic nerve (V1), the maxillary nerve (V2), and the mandibular nerve (V3). | |
| Classification and external resources | |
| Specialty | Neurology |
| ICD-10 | G50.0, G44.847 |
| ICD-9-CM | 350.1 |
| DiseasesDB | 13363 |
| MedlinePlus | 000742 |
| eMedicine | emerg/617 |
| MeSH | D014277 |

Trigeminal neuralgia (TN or TGN) is a chronic pain disorder that affects the trigeminal nerve. There are two main types: typical and atypical trigeminal neuralgia. The typical form results in episodes of severe, sudden, shock like pain in one side of the face that lasts for seconds to a few minutes. Groups of these episodes can occur over a few hours. The atypical form results in a constant burning pain that is less severe. Episodes may be triggered by any touch to the face. Both forms may occur in the same person.[1] It is one of the most painful conditions and can result in depression.[5]
The exact cause is unclear but believed to involve loss of the myelin around the trigeminal nerve.[1][6] This may occur due to compression from a blood vessel as the nerve exits the brain stem, multiple sclerosis, stroke, or trauma. Less common causes include a tumor or arteriovenous malformation. It is a type of nerve pain. Diagnosis is typically based on the symptoms after ruling out other possible causes such as postherpetic neuralgia.[1]
Treatment includes medication or surgery.[1] The anticonvulsant carbamazepine or oxcarbazepine is the usual initial treatment and is effective in about 80% of people. Other options include lamotrigine, baclofen, gabapentin, and pimozide.[6] Amitriptyline may help with the pain but opioids are not usually effective in the typical form.[1] In those who do not improve or become resistant to other measures, a number of types of surgery may be tried.[6]
It is estimated that 1 in 8,000 people develop trigeminal neuralgia a year. It usually begins in people over 50 years old, but can occur at any age. Women are more commonly affected than men.[1] The condition was first described in detail in 1773 by John Fothergill.[7]
Signs and symptoms
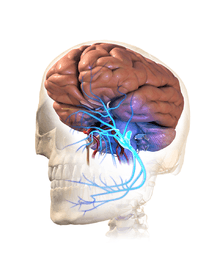
This disorder is characterized by episodes of intense facial pain along the trigeminal nerve divisions. The trigeminal nerve is a paired cranial nerve that has three major branches: the ophthalmic nerve (V1), the maxillary nerve (V2), and the mandibular nerve (V3). One, two, or all three branches of the nerve may be affected. Trigeminal neuralgia most commonly involves the middle branch (the maxillary nerve or V2) and lower branch (mandibular nerve or V3) of the trigeminal nerve.[8]
Individual attack usually lasts from a few seconds to several minutes or hours, but these can repeat for hours with very short intervals between attacks. In other instances only 4-10 attacks are experienced daily. The episodes of intense pain may occur paroxysmally. To describe the pain sensation, people often describe a trigger area on the face so sensitive that touching or even air currents can trigger an episode; however, in many people the pain is generated spontaneously without any apparent stimulation. It affects lifestyle as it can be triggered by common activities such as eating, talking, shaving and brushing teeth. Wind, chewing and talking can aggravate the condition in many patients. The attacks are said by those affected to feel like stabbing electric shocks, burning, sharp, pressing, crushing, exploding or shooting pain that becomes intractable.
The pain also tends to occur in cycles with remissions lasting months or even years. 1–6% of cases occur on both sides of the face but extremely rare for both to be affected at the same time.[9] This normally indicates problems with both trigeminal nerves, since one serves strictly the left side of the face and the other serves the right side. Pain attacks are known to worsen in frequency or severity over time, in some people. Pain may migrate to other branches over time but in some people remains very stable.[10]
Rapid spreading of the pain, bilateral involvement or simultaneous participation with other major nerve trunks (such as Painful Tic Convulsif of nerves V & VII or occurrence of symptoms in the V and IX nerves) may suggest a systemic cause. Systemic causes could include multiple sclerosis or expanding cranial tumours.[11]
The severity of the pain makes it difficult to wash the face, shave, and perform good oral hygiene. The pain has a significant impact on activities of daily living especially as people live in fear of when they are going to get their next attack of pain and how severe it will be. It can lead to severe depression and anxiety.[12]
However, not all people will have the symptoms described above and there are variants of TN. One of which is atypical trigeminal neuralgia ("trigeminal neuralgia, type 2" or trigeminal neuralgia with concomitant pain ),[13] based on a recent classification of facial pain.[14] In these instances there is also a more prolonged lower severity background pain that can be present for over 50% of the time and is described more as a burning or prickling, rather than a shock.
Trigeminal neuropathic pain is similar to TN2 but can have the electric pulses associated with classic TN. The pain is usually constant and can also give off a tingling, numbness sensation. This pain is due to unintentional damage to one or more of the trigeminal nerves from trauma, oral surgery, dentistry work, etc. It is difficult to treat but sufferers are usually given the same anticonvulsant and tricyclics antidepressant medicines as with the other types of neuralgias. Surgical options are DREZ (dorsal root entry zone) lesion and MCS or Motor Cortex Stimulation.
TN needs to be distinguished from other forms of unilateral pain which is related to damage to the trigeminal nerve by trauma to the face or dental treatments. This is often termed painful trigeminal neuropathy or post-traumatic neuropathy as some sensory changes can be noted e.g. decrease in pain sensation or temperature. This is important as different care pathways are used. Trigeminal pain can also occur after an attack of herpes zoster, and post-herpetic neuralgia has the same manifestations as in other parts of the body. Trigeminal deafferentation pain (TDP), also termed anaesthesia dolorosa, is from intentional damage to a trigeminal nerve following attempts to surgically fix a nerve problem. This pain is usually constant with a burning sensation and numbness. TDP is very difficult to treat as further surgeries are usually ineffective and possibly detrimental to the person.
Causes
The trigeminal nerve is a mixed cranial nerve responsible for sensory data such as tactition (pressure), thermoception (temperature), and nociception (pain) originating from the face above the jawline; it is also responsible for the motor function of the muscles of mastication, the muscles involved in chewing but not facial expression.
Several theories exist to explain the possible causes of this pain syndrome. It was once believed that the nerve was compressed in the opening from the inside to the outside of the skull; but leading research indicates that it is an enlarged or lengthened blood vessel – most commonly the superior cerebellar artery – compressing or throbbing against the microvasculature of the trigeminal nerve near its connection with the pons.[15] Such a compression can injure the nerve's protective myelin sheath and cause erratic and hyperactive functioning of the nerve. This can lead to pain attacks at the slightest stimulation of any area served by the nerve as well as hinder the nerve's ability to shut off the pain signals after the stimulation ends. This type of injury may rarely be caused by an aneurysm (an outpouching of a blood vessel); by an AVM (arteriovenous malformation);[16] by a tumor; such as an arachnoid cyst or meningioma in the cerebellopontine angle;[17] or by a traumatic event such as a car accident.[18]
Short-term peripheral compression is often painless.[5] Persistent compression results in local demyelination with no loss of axon potential continuity. Chronic nerve entrapment results in demyelination primarily, with progressive axonal degeneration subsequently.[5] It is, "therefore widely accepted that trigeminal neuralgia is associated with demyelination of axons in the Gasserian ganglion, the dorsal root, or both."[19] It has been suggested that this compression may be related to an aberrant branch of the superior cerebellar artery that lies on the trigeminal nerve.[19] Further causes, besides an aneurysm, multiple sclerosis or cerebellopontine angle tumor, include: a posterior fossa tumor, any other expanding lesion or even brainstem diseases from strokes.[19]
Trigeminal neuralgia is found in 3–4% of people with multiple sclerosis, according to data from seven studies.[20][21] It has been theorized that this is due to damage to the spinal trigeminal complex.[22] Trigeminal pain has a similar presentation in patients with and without MS.[23]
Postherpetic neuralgia, which occurs after shingles, may cause similar symptoms if the trigeminal nerve is damaged.
When there is no [apparent] structural cause, the syndrome is called idiopathic.
Management
As with many conditions without clear physical or laboratory diagnosis, TN is sometimes misdiagnosed. A TN sufferer will sometimes seek the help of numerous clinicians before a firm diagnosis is made.
There is evidence that points towards the need to quickly treat and diagnose TN. It is thought that the longer a patient suffers from TN, the harder it may be to reverse the neural pathways associated with the pain.
The differential diagnosis includes temporomandibular disorder.[24] Since triggering may be caused by movements of the tongue or facial muscles, TN must be differentiated from masticatory pain that has the clinical characteristics of deep somatic rather than neuropathic pain. Masticatory pain will not be arrested by a conventional mandibular local anesthetic block.[11] One quick test a dentist might perform is a conventional inferior dental local anaesthetic block, if the pain is in this branch, as it will not arrest masticatory pain but will TN.[25]
Medical
- The anticonvulsant carbamazepine is the first line treatment; second line medications include baclofen, lamotrigine, oxcarbazepine, phenytoin, gabapentin and pregabalin. Uncontrolled trials have suggested that clonazepam and lidocaine may be effective.[26]
- Antidepressant medications, such as amitriptyline have shown good efficacy in treating trigeminal neuralgia, especially if combined with an anti-convulsant drug such as pregabalin.[27]
- There is some evidence that duloxetine can also be used in some cases of neuropathic pain, especially in patients with major depressive disorder[28] as it is an antidepressant. However, it should, by no means, be considered a first line therapy and should only be tried by specialist advice.[29]
- There is a lot of controversy around opiate use such as morphine and oxycodone for treatment of TN, with varying evidence on its effectiveness for neuropathic pain. Generally, opioids are considered ineffective against TN and thus should not be prescribed.[30]
Surgical
The evidence for surgical therapy is extensive[31] and surgery is normally recommended only after medical treatment has proved ineffective, or if side effects of medication are intolerable.[32] While there may be pain relief there is also frequently numbness post procedure.[31] Microvascular decompression appears to result in the longest pain relief.[31][33] Percutaneous radiofrequency thermorhizotomy may also be effective[34] as may stereotactic radiosurgery, however the effectiveness decreases with time.[35]
Surgical procedures can be separated into non-destructive and destructive:
Non Destructive:
- Microvascular decompression - this involves a small incision behind the ear and some bone removal from the area. An incision through the meninges is made to expose the nerve. Any vascular compressions of the nerve are carefully moved and a sponge-like pad is placed between the compression and nerve, stopping unwanted pulsation and allowing myelin sheath healing. This technique appears to result in the longest pain relief.[31]
Destructive: All destructive procedures will cause facial numbness, post relief, as well as pain relief.[31]
- Percutaneous techniques which all involve a needle or catheter entering the face up to the origin where the nerve splits into three divisions and then damaging this area, purposely, to produce numbness but also stop pain signals. These techniques are proven effective[34] especially in those where other interventions have failed or in those who are medically unfit for surgery such as the elderly.
- Balloon compression - inflation of a balloon at this point causing damage and stopping pain signals.
- Glycerol injection- deposition of a corrosive liquid called glycerol at this point causes damage to the nerve to hinder pain signals.
- Radiofrequency thermocoagulation rhizotomy - application of a heated needle to damage the nerve at this point.
- Stereotactic radiosurgery or “Gamma Knife Surgery” is a form of radiation therapy that focuses high-power energy on a small area of the body[36]
Support
Psychological and social support has found to play a key role in the management of chronic illnesses and chronic pain conditions, such as trigeminal neuralgia. Chronic pain can cause constant frustration to an individual as well as to those around them.[37] As a result, there are many advocacy groups.
History
Trigeminal neuralgia was first described by physician John Fothergill and treated surgically by John Murray Carnochan, both of whom were graduates of the University of Edinburgh Medical School. Historically TN has been called "suicide disease" due to studies by Dr Harvey Cushing which demonstrated 0.6% mortality involving 123 cases of TN during 1896 and 1912.[4][40]
Society and culture
Some individuals of note with TN include:
- Entrepreneur and author Melissa Seymour was diagnosed with TN in 2009 and underwent microvascular decompression surgery in a well documented case covered by magazines and newspapers which helped to raise public awareness of the illness in Australia. Seymour was subsequently made a Patron of the Trigeminal Neuralgia Association of Australia.[41]
- Salman Khan, one of India's biggest film stars, was diagnosed with TN in 2011, resulting in tremendous media coverage in the country and abroad. He underwent surgery in the US.[42]
- All-Ireland winning Gaelic footballer Christy Toye was diagnosed with the condition in 2013. He spent five months in his bedroom at home, returned for the 2014 season and lined out in another All-Ireland final with his team.[43]
- Jim Fitzpatrick - Member of Parliament for Poplar and Limehouse - disclosed he suffered from trigeminal neuralgia before undergoing neurosurgery. He has openly discussed his condition at parliamentary meetings and is a prominent figure in the TNA UK charity.[44]
- Andrea Jenkyns - Member of Parliament for Morley and Outwood - diagnosis with TN came to light during her television debate on Prime Minister’s Questions where she struggled to get her words out.[45]
- Jefferson Davis - President of the Confederate States of America [46]
- Charles Sanders Peirce - American philosopher, scientist and father of pragmatism. (Joseph Brent, Charles Sanders Peirce: A Life [Bloomington: Indiana University Press, 1993] p. 39-40)
- Gloria Steinem - American feminist, journalist, and social and political activist [47]
- Anneli van Rooyen, Afrikaans singer-songwriter popular during the 1980s and 1990s, was diagnosed with atypical trigeminal neuralgia in 2004. During surgical therapy directed at alleviating the condition performed in 2007, Van Rooyen suffered permanent nerve damage, resulting in her near-complete retirement from performing.[48]
Research directions
- Gallium maltolate in a cream or ointment base has been studied in a case report as a treatment of refractory postherpetic trigeminal neuralgia.[49]
See also
References
- 1 2 3 4 5 6 7 "Trigeminal Neuralgia Fact Sheet". NINDS. November 3, 2015. Retrieved 1 October 2016.
- ↑ Hackley, CE (1869). A text-book of practical medicine. D. Appleton & Co. p. 292. Retrieved 2011-08-01.
- ↑ Bagheri, SC; et al. (December 1, 2004). "Diagnosis and treatment of patients with trigeminal neuralgia". Journal of the American Dental Association. 135 (12): 1713–7. doi:10.14219/jada.archive.2004.0124. PMID 15646605. Retrieved 2011-08-01.
- 1 2 Adams, H; Pendleton, C; Latimer, K; Cohen-Gadol, AA; Carson, BS; Quinones-Hinojosa, A (May 2011). "Harvey Cushing's case series of trigeminal neuralgia at the Johns Hopkins Hospital: a surgeon's quest to advance the treatment of the 'suicide disease'.". Acta neurochirurgica. 153 (5): 1043–50. doi:10.1007/s00701-011-0975-8. PMID 21409517.
- 1 2 3 Okeson, JP (2005). "6". In Lindsay Harmon. Bell's orofacial pains: the clinical management of orofacial pain. Quintessence Publishing Co, Inc. p. 114. ISBN 0-86715-439-X.
- 1 2 3 Obermann, Mark (2010-03-01). "Treatment options in trigeminal neuralgia". Therapeutic Advances in Neurological Disorders. 3 (2): 107–115. doi:10.1177/1756285609359317. ISSN 1756-2856. PMC 3002644
 . PMID 21179603.
. PMID 21179603. - ↑ Prasad, S; Galetta, S (March 2009). "Trigeminal neuralgia: historical notes and current concepts.". The neurologist. 15 (2): 87–94. PMID 19276786.
- ↑ Trigeminal neuralgia and hemifacial spasm Archived February 15, 2012, at the Wayback Machine. by UF&Shands – The University of Florida Health System. Retrieved Mars 2012
- ↑ Raval AB, Salluzzo J, Dvorak T, Price LL, Mignano JE, Wu JK (2014). "Salvage Gamma Knife Radiosurgery after failed management of bilateral trigeminal neuralgia". Surg Neurol Int. 5: 160. doi:10.4103/2152-7806.145201. PMC 4258705. PMID 25525553.
- ↑ Bayer DB, Stenger TG (1979). "Trigeminal neuralgia: an overview". Oral Surg Oral Med Oral Pathol. 48 (5): 393–9. doi:10.1016/0030-4220(79)90064-1. PMID 226915.
- 1 2 Okeson, JP (2005). "17". In Lindsay Harmon. Bell's orofacial pains: the clinical management of orofacial pain. Quintessence Publishing Co, Inc. p. 453. ISBN 0-86715-439-X.
- ↑ "The psychosocial and affective burden of posttraumatic neuropathy following injuries to the trigeminal nerve.". J Orofac Pain. 27: 293–303. 2013. doi:10.11607/jop.1056. PMID 24171179.
- ↑ "Neurological surgery: facial pain". Oregon Health & Science University. Retrieved 2011-08-01.
- ↑ Burchiel KJ (2003). "A new classification for facial pain". Neurosurgery. 53 (5): 1164–7. doi:10.1227/01.NEU.0000088806.11659.D8. PMID 14580284.
- ↑ Nurmikko, T. J.; Eldridge, P. R (2009). "Trigeminal neuralgia—pathophysiology, diagnosis and current treatment". Pain (87): 165–166.
- ↑ Singh N, Bharatha A, O’Kelly C, Wallace MC, Goldstein W, Willinsky RA, Aviv RI, Symons SP. Intrinsic arteriovenous malformation of the trigeminal nerve. Canadian Journal of Neurological Sciences. 2010 September; 37(5):681–683.
- ↑ Babu R, Murali R (1991). "Arachnoid cyst of the cerebellopontine angle manifesting as contralateral trigeminal neuralgia: case report". Neurosurgery. 28 (6): 886–7. doi:10.1097/00006123-199106000-00018. PMID 2067614.
- ↑ Croft, Stephen M. Foreman, Arthur C. (2002). Whiplash injuries : the cervical acceleration/deceleration syndrome (3rd ed.). Baltimore: Williams & Wilkins. p. 481. ISBN 9780781726818.
- 1 2 3 Okeson, JP (2005). "6". In Lindsay Harmon. Bell's orofacial pains: the clinical management of orofacial pain. Quintessence Publishing Co, Inc. p. 115. ISBN 0-86715-439-X.
- ↑ Foley P, Vesterinen H, Laird B, et al. (2013). "Prevalence and natural history of pain in adults with multiple sclerosis: Systematic review and meta-analysis". Pain. 154 (5): 632–42. doi:10.1016/j.pain.2012.12.002. PMID 23318126.
- ↑ De Santi, L; Annunziata, P (February 2012). "Symptomatic cranial neuralgias in multiple sclerosis: Clinical features and treatment". Clinical Neurology and Neurosurgery. 114 (2): 101–7. doi:10.1016/j.clineuro.2011.10.044.
- ↑ Cruccu G, Biasiotta A, Di Rezze S, et al. (2009). "Trigeminal neuralgia and pain related to multiple sclerosis". Pain. 143 (3): 186–91. doi:10.1016/j.pain.2008.12.026. PMID 19171430.
- ↑ De Simone R, Marano E, Brescia MV, et al. (2005). "A clinical comparison of trigeminal neuralgic pain in patients with and without underlying multiple sclerosis". Neurol Sci. 26 Suppl 2: s150–1. doi:10.1007/s10072-005-0431-8. PMID 15926016.
- ↑ Drangsholt, M; Truelove, EL (2001). "Trigeminal neuralgia mistaken as temporomandibular disorder". J Evid Base Dent Pract. 1 (1): 41–50. doi:10.1067/med.2001.116846.
- ↑ Cherian, Anusha. "Dr". MedScape. Retrieved 20 November 2015.
- ↑ Sindrup, SH; Jensen, TS (2002). "Pharmacotherapy of trigeminal neuralgia". Clin J Pain. 18 (1): 22–7. doi:10.1097/00002508-200201000-00004. PMID 11803299.
- ↑ Lawal, Ahmed; et al. (September 2012). "Management of Trigeminal Neuralgia using Amitriptyline and Pregablin combination Therapy". African Journal of Biomedical Research. 15 (1): 201–203.
- ↑ Hsu, CC; et al. (Apr 2014). "Rapid Management of Trigeminal Neuralgia and Comorbid Major Depressive Disorder With Duloxetine.". Annals of Pharmacotherapy. 30;48 (8): 1090–1092.
- ↑ Lunn, MPT; Hughes, R.A.C; Wiffen, P.J (7 October 2009). "Duloxetine for treating painful neuropathy or chronic pain". In Lunn, MPT. Duloxetine for treating painful neuropathy or chronic pain. The Cochrane Database of Systematic Reviews. doi:10.1002/14651858.CD007115.pub2. Retrieved 2011-08-01.
- ↑ Raymond, Sekula. "Dr". Neurological Surgery - University of Pittsburgh. University of Pittsburgh. Retrieved 20 November 2015.
- 1 2 3 4 5 Zakrzewska, JM; Akram, H (Sep 7, 2011). "Neurosurgical interventions for the treatment of classical trigeminal neuralgia.". Cochrane database of systematic reviews (Online). 9: CD007312. doi:10.1002/14651858.CD007312.pub2. PMID 21901707.
- ↑ Sindou, M; Keravel, Y (April 2009). "[Algorithms for neurosurgical treatment of trigeminal neuralgia].". Neuro-Chirurgie. 55 (2): 223–5. doi:10.1016/j.neuchi.2009.02.007. PMID 19328505.
- ↑ 2015 review of treatment of TN
- 1 2 Sindou, M; Tatli, M (April 2009). "[Treatment of trigeminal neuralgia with thermorhizotomy].". Neuro-Chirurgie. 55 (2): 203–10. doi:10.1016/j.neuchi.2009.01.015. PMID 19303114.
- ↑ Dhople, AA; Adams, JR; Maggio, WW; Naqvi, SA; Regine, WF; Kwok, Y (August 2009). "Long-term outcomes of Gamma Knife radiosurgery for classic trigeminal neuralgia: implications of treatment and critical review of the literature. Clinical article.". Journal of Neurosurgery. 111 (2): 351–8. doi:10.3171/2009.2.JNS08977. PMID 19326987.
- ↑ Yi-Bin, Chen. MedLine Plus https://www.nlm.nih.gov/medlineplus/ency/article/007274.htm. Retrieved 20 November 2015. Missing or empty
|title=(help) - ↑ Molitor, Nancy. "Dr". American Psychological Association. APA. Retrieved 27 June 2015.
- ↑ Williams, Christopher; Dellon, A.; Rosson, Gedge (5 March 2009). "Management of Chronic Facial Pain". Craniomaxillofacial Trauma and Reconstruction. 2 (02): 067–076. doi:10.1055/s-0029-1202593. PMC 3052669. PMID 22110799.
- ↑ "Facial Neuralgia Resources". Trigeminal Neuralgia Resources / Facial Neuralgia Resources. Retrieved 8 May 2013.
- ↑ Prasad, S; Galetta, S (2009). "Trigeminal Neuralgia Historical Notes and Current Concept". Neurologist. 15 (2): 87–94. doi:10.1097/NRL.0b013e3181775ac3. PMID 19276786.
- ↑ "Melissa Seymour: My perfect life is over". Womansday.ninemsn.com.au. 2009-06-18. Archived from the original on 2009-12-14. Retrieved 2013-10-09.
- ↑ "Salman suffering from the suicide disease". http://www.hindustantimes.com. 2011-08-24. Archived from the original on 2014-07-15. Retrieved 2014-06-18. External link in
|publisher=(help) - ↑ Foley, Alan (16 September 2014). "Serious illness meant Christy Toye didn't play in 2013 but now he's set for All-Ireland final: The Donegal player has experienced a remarkable revival". The Score. Archived from the original on 4 October 2014. Retrieved 16 September 2014.
- ↑ "MP urges greater awareness of trigeminal neuralgia". BBC - Democracy Live. BBC. Retrieved 20 November 2015.
- ↑ Swerling, Gabriella. "MP blames Scream disorder for 'nerves'". The Times. The Times. Retrieved 20 November 2015.
- ↑ http://www.senate.gov/artandhistory/history/minute/Jefferson_Davis_Farewell.htm
- ↑ Gorney, Cynthia (November–December 1995). "Gloria". Mother Jones. Retrieved July 1, 2016.
- ↑ "Anneli van Rooyen's road to recovery". Retrieved 2016-09-12.
- ↑ Bernstein, L.R. (2013). "Gallium, therapeutic effects" (PDF). In Kretsinger, R.H.; Uversky, V.N.; Permyakov, E.A. Encyclopedia of Metalloproteins. New York: Springer. pp. 823–835. ISBN 978-1-4614-1532-9.