Erythema nodosum
| Erythema nodosum | |
|---|---|
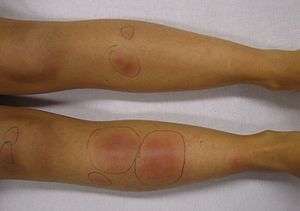 | |
| Erythema nodosum in a person who had recently had streptococcal pharyngitis | |
| Classification and external resources | |
| Specialty | Dermatology, rheumatology |
| ICD-10 | L52 |
| ICD-9-CM | 695.2, 017.1 |
| DiseasesDB | 4462 |
| MedlinePlus | 000881 |
| eMedicine | derm/138 |
| MeSH | D004893 |
Erythema nodosum (EN) is an inflammatory condition characterised by inflammation of the fat cells under the skin, resulting in tender red nodules or lumps that are usually seen on both shins. It can be caused by a variety of conditions, and typically resolves spontaneously within 30 days.[1] It is common in young people between 12–20 years of age.
Signs and symptoms


Pre-eruptive phase
The first sign of erythema nodosum is often flu-like symptoms.[2] It may involve a pyrexia, weakness and arthralgia.
Eruptive stage
It is characterized by the appearance of dermo-hypodermic rounded nodules which may be bright red or purplish, bilaterally symmetrical, located on the extensor surface of the legs. They are movable relative to the deep plane and skin. They generally disappear in 1–6 weeks without sequelae.
Erythema nodosum is characterised by red nodules that are tender and warm.[3] Nodules occur under the skin, classically in front of the shins. Nodules may occur anywhere there is fat under the skin, including the thighs, arms, trunk, face, and neck.[3]
Erythema nodosum may occur concurrently with fever, malaise, and joint pain and inflammation.[3] Nodules vary from 1–10 cm in diameter, and may coalesce to form large areas of hardened skin.[4]
As the nodules age, they become bluish purple, brownish, yellowish, and finally green, similar to the color changes that occur in a resolving bruise. The nodules usually subside over a period of 2–6 weeks without ulceration or scarring.[5]
Less common variants of erythema nodosum include:
- Ulcerating forms, seen in Crohn's disease [3]
- Erythema contusiforme, an erythema nodosum lesion with subcutaneous haemorrhage [3]
- Chronic erythema nodosum, more likely to be unilateral and migratory.[3]
- Erythema nodosum migrans, (also known as subacute nodular migratory panniculitis of Vilanova and Piñol), a form of erythema nodosum with lesions that spread centrifugally with central clearing,[3] and a form of chronic erythema nodosum.[6]) is a form of septal panniculitis that is much less common than acute erythema nodosum.[7]:488
- Lofgren's syndrome, a form of acute sarcoidosis with erythema nodosum, bilateral hilar adenopathy and fever, often accompanied by joint symptoms.
Causes
EN is associated with a wide variety of conditions, including:
- Idiopathic
In about 30–50% of cases, the cause of EN is unknown.[8]
- Infection[4]
- Streptococcal infection which, in children, is by far the most common precipitant,[7]:488
- Primary infection of Tuberculosis
- Mycoplasma pneumoniae
- Histoplasma capsulatum
- Yersinia
- Epstein-Barr virus
- Coccidioides immitis (Valley fever)
- Cat scratch disease
- Autoimmune disorders, including[3]
- Sulfonamides
- Penicillins
- Oral contraceptives
- Bromides
- Hepatitis B vaccination[10]
- Cancer, including[3]
EN may also be due to excessive antibody production in lepromatous leprosy leading to deposition of immune complexes.[11]
There is an association with the HLA-B27 histocompatibility antigen, which is present in 65% of patients with erythema nodosum.[12]
A useful mnemonic for causes is SORE SHINS (Streptococci, OCP, Rickettsia, Eponymous (Behçet), Sulfonamides, Hansen's Disease (Leprosy), IBD, NHL, Sarcoidosis.[13]
Pathophysiology
Erythema nodosum is probably a delayed hypersensitivity reaction to a variety of antigens. Although circulating immune complexes have been demonstrated in patients with inflammatory bowel disease, they have not been found in idiopathic or uncomplicated cases.[14]
Diagnosis
Erythema nodosum is diagnosed clinically. A biopsy can be taken and examined microscopically to confirm an uncertain diagnosis.[5]:148 Microscopic examination usually reveals a neutrophilic infiltrate surrounding capillaries that results in septal thickening, with fibrotic changes in the fat around blood vessels. A characteristic microscopic finding is radial granulomas, well-defined nodular aggregates of histiocytes surrounding a stellate cleft.[4]
Additional evaluation should be performed to determine the underlying cause of erythema nodosum. This may include a full blood count, erythrocyte sedimentation rate (ESR), antistreptolysin-O (ASO) titer and throat culture, urinalysis, intradermal tuberculin test, and a chest x-ray.[15] The ESR is typically high, the C-reactive protein elevated, and the blood showing an increase in white blood cells.[5]:148
The ESR is initially very high, and falls as the nodules of erythema nodosum. The ASO titer is high in cases associated with a streptococcal throat infection. A chest X-ray should be performed to rule out pulmonary diseases, in particular sarcoidosis and Löfgren syndrome.[5]:148
Treatment
Erythema nodosum is self-limiting and usually resolves itself within 3–6 weeks. A recurring form does exist, and in children it is attributed to repeated infections with streptococcus.[11] Treatment should focus on the underlying cause. Symptoms can be treated with bedrest, leg elevation, compressive bandages, wet dressings, and nonsteroidal anti-inflammatory agents (NSAIDs).[4] NSAIDs are usually more effective at the onset of EN versus with chronic disease.
Potassium iodide can be used for persistent lesions whose cause remains unknown. Corticosteroids and colchicine can be used in severe refractory cases.[16][17] Thalidomide has been used successfully in the treatment of Erythema nodosum leprosum,[18] and it was approved by the U.S. FDA for this use in July 1998.[19]
Epidemiology
Erythema nodosum is the most common form of panniculitis. It is most common in the ages of 20–30, and affects women 3–6 times more than men.[5]:148
About 15 percent of patients with inflammatory bowel disease develop erythema nodosum.[20]
References
- ↑ Pedro-Pons, Agustín (1968). Patología y Clínica Médicas (in Spanish). 6 (3rd ed.). Barcelona: Salvat. p. 193. ISBN 84-345-1106-1.
- ↑ Erythema nodosum information http://www.gosh.nhs.uk/medical-information/search-for-medical-conditions/erythema-nodosum/erythema-nodosum-information/
- 1 2 3 4 5 6 7 8 9 10 11 Gilchrist, H; Patterson, JW (Jul–Aug 2010). "Erythema nodosum and erythema induratum (nodular vasculitis): diagnosis and management". Dermatologic therapy. 23 (4): 320–7. doi:10.1111/j.1529-8019.2010.01332.x. PMID 20666819.
- 1 2 3 4 Schwartz, RA; Nervi, SJ (Mar 1, 2007). "Erythema nodosum: a sign of systemic disease". American family physician. 75 (5): 695–700. PMID 17375516.
- 1 2 3 4 5 Fitzpatrick, Thomas B. (2005). Fitzpatrick's color atlas and synopsis of clinical dermatology (5th ed.). New York: McGraw-Hill Medical Pub. Division. ISBN 0-07-144019-4.
- ↑ Rapini, Ronald P.; Bolognia, Jean L.; Jorizzo, Joseph L. (2007). Dermatology: 2-Volume Set. St. Louis: Mosby. ISBN 1-4160-2999-0.
- 1 2 William D. James; Timothy G. Berger; Dirk M. Elston. Andrews' Diseases of the skin : clinical dermatology. (11th ed.). [London]: Saunders/ Elsevier. ISBN 1437703143.
- 1 2 Mert, A; Ozaras, R; Tabak, F; Pekmezci, S; Demirkesen, C; Ozturk, R (2004). "Erythema nodosum: an experience of 10 years". Scandinavian journal of infectious diseases. 36 (6–7): 424–7. doi:10.1080/00365540410027184. PMID 15307561.
- ↑ Bohn S, Buchner S, Itin P (1997). "Erythema nodosum: 112 cases. Epidemiology, clinical aspects and histopathology". Schweiz Med Wochenschr. 127 (27–28): 1168–76. PMID 9324739.
- ↑ Rogerson SJ, Nye FJ (1990-08-11). "Hepatitis B vaccine associated with erythema nodosum and polyarthritis" (PDF). BMJ. 301 (6747): 345. doi:10.1136/bmj.301.6747.345. PMC 1663612
 . PMID 2144199.
. PMID 2144199. - 1 2 Kumar V, Abbas A (2009). Robbins and Coltran Pathological Basis of Disease. pp. 372–373. ISBN 978-1416049302.
- ↑ Cunha, Burke A. (1999). Infectious disease pearls. Philadelphia: Hanley & Belfus. p. 105. ISBN 978-1560532033.
- ↑ Dr Kevin McCarthy, Cork, Ireland or DIPOUT: Drugs (e.g. sulfonamides), Infections (e.g. strep), Pregnancy, OCP, Ulcerative colitis, TB
- ↑ Nguyen, GC; Torres, EA; Regueiro, M; Bromfield, G; Bitton, A; Stempak, J; Dassopoulos, T; Schumm, P; Gregory, FJ; Griffiths, AM; Hanauer, SB; Hanson, J; Harris, ML; Kane, SV; Orkwis, HK; Lahaie, R; Oliva-Hemker, M; Pare, P; Wild, GE; Rioux, JD; Yang, H; Duerr, RH; Cho, JH; Steinhart, AH; Brant, SR; Silverberg, MS (May 2006). "Inflammatory bowel disease characteristics among African Americans, Hispanics, and non-Hispanic Whites: characterization of a large North American cohort". The American journal of gastroenterology. 101 (5): 1012–23. doi:10.1111/j.1572-0241.2006.00504.x. PMID 16696785.
- ↑ García-Porrúa, C; González-Gay, MA; Vázquez-Caruncho, M; López-Lazaro, L; Lueiro, M; Fernández, ML; Alvarez-Ferreira, J; Pujol, RM (March 2000). "Erythema nodosum: etiologic and predictive factors in a defined population". Arthritis and rheumatism. 43 (3): 584–92. doi:10.1002/1529-0131(200003)43:3<584::AID-ANR15>3.0.CO;2-6. PMID 10728752.
- ↑ Mat C, Yurdakul S, Uysal S, Gogus F, Ozyazgan Y, Uysal O, Fresko I, Yazici H (2005). "A double-blind trial of depot corticosteroids in Behcet's syndrome". Rheumatology (Oxford). 45 (3): 348–52. doi:10.1093/rheumatology/kei165. PMID 16263779.
- ↑ Yurdakul S, Mat C, Tuzun Y, Ozyazgan Y, Hamuryudan V, Uysal O, Senocak M, Yazici H (2001). "A double-blind trial of colchicine in Behcet's syndrome". Arthritis Rheum. 44 (11): 2686–92. doi:10.1002/1529-0131(200111)44:11<2686::AID-ART448>3.0.CO;2-H. PMID 11710724.
- ↑ Silverman WA (August 2002). "The schizophrenic career of a "monster drug"". Pediatrics. 110 (2 Pt 1): 404–6. doi:10.1542/peds.110.2.404. PMID 12165600.
- ↑ Rouhi, Maureen. "Thalidomide". Chemical & Engineering News. American Chemical Society. Retrieved 2006-09-21.
- ↑ Goldman, Lee. Goldman's Cecil Medicine (24th ed.). Philadelphia: Elsevier Saunders. p. 915. ISBN 1437727883.
| Wikimedia Commons has media related to Erythema nodosum. |