General Behavior Inventory
| Psychology |
|---|
| Basic types |
| Applied psychology |
| Lists |
|
| Richard Allen Depue, Ph.D. | |
|---|---|
| Occupation | Professor |
| Known for | Authoring the General Behavior Inventory; investigating the neurobiology underlying major personality traits |
The General Behavior Inventory (GBI) is a 73-question psychological self-report assessment tool designed by Richard Depue[1] and colleagues to identify the presence and severity of manic and depressive moods in adults, as well as to assess for cyclothymia. It is one of the most widely used psychometric tests for measuring the severity of bipolar disorder and the fluctuation of symptoms over time. The GBI is intended to be administered for adult populations; however, it has been adapted into versions that allow for juvenile populations (for parents to rate their offspring), as well as a short version that allows for it to be used as a screening test.
Versions
Parent GBI (P-GBI)
The P-GBI [2] is an adaptation of the GBI, consisting of 73 Likert scale items rated on a scale from 0 ("Never or Hardly Ever") to 3 ("Very often or Almost Constantly"). It consists of two scales: a depressive symptoms (46 items) and a hypomanic/biphasic (mixed) symptoms (28 items).[3]
Parent GBI-10-Item Mania Scale (PGBI-10M)
The PGBI-10M [3] is a brief (10-item) version of the PGBI that was validated for clinical use for patients presenting with a variety of different diagnoses, including frequent comorbid conditions. It is administered to parents for them to rate their children between ages 5–17. The 10 items include symptoms such as elated mood, high energy, irritability and rapid changes in mood and energy as indicators of potential juvenile bipolar disorder.[3]
7 Up 7 Down Inventory (7U7D)
The 7U7D [4] is a 14-item measure of manic and depressive tendencies that was carved from the full length GBI. This version is designed to be applicable for both youths and adults, and to improve separation between both mania and depressive conditions. It was developed via factor analysis from nine separate samples pooled into two age groups, ensuring applicability for use in youth and adults.[4]
Psychometric properties
The GBI has been used extensively in research, including clinical samples, college students, longitudinal, treatment, and other studies. However, no normative data exist to calibrate scores in the general population.
Reliability
The GBI has exceptionally high internal consistency because it has long scales with a large number of items . The GBI shows high reliability whether completed as a self report or as a caregiver report about youth behavior .
Retest reliability also is good over a week or two week period, although the GBI's length makes it tedious to complete frequently .
| Criterion | Rating (adequate, good, excellent, too good*) | Explanation with references |
|---|---|---|
| Norms | Adequate | Multiple convenience samples and research studies, including both clinical and nonclinical samples |
| Internal consistency (Cronbach’s alpha, split half, etc.) | Excellent; too good for some contexts | Alphas routinely over .94 for both scales, suggesting that scales could be shortened for many uses |
| Inter-rater reliability | Not applicable | Designed originally as a self-report scale; parent and youth report correlate about the same as cross-informant scores correlate in general[5] |
| Test-retest reliability (stability | Good | r = .73 over 15 weeks. Evaluated in initial studies,[6] with data also show high stability in clinical trials |
| Repeatability | Not published | No published studies formally checking repeatability |
Validity
| Criterion | Rating (adequate, good, excellent, too good*) | Explanation with references |
|---|---|---|
| Content validity | Excellent | Covers both DSM diagnostic symptoms and a range of associated features[6] |
| Construct validity (e.g., predictive, concurrent, convergent, and discriminant validity) | Excellent | Shows convergent validity with other symptom scales, longitudinal prediction of development of mood disorders,[7][8][9] criterion validity via metabolic markers[6][10] and associations with family history of mood disorder.[11] Factor structure complicated;[6][12] the inclusion of “biphasic” or “mixed” mood items creates a lot of cross-loading |
| Discriminative validity | Excellent | Multiple studies show that GBI scores discriminate cases with unipolar and bipolar mood disorders from other clinical disorders[6][13][14] effect sizes are among the largest of existing scales[15] |
| Validity generalization | Good | Used both as self-report and caregiver report; used in college student[12][16] as well as outpatient[13][17][18] and inpatient clinical samples; translated into multiple languages with good reliability |
| Treatment sensitivity | Good | Multiple studies show sensitivity to treatment effects comparable to using interviews by trained raters, including placebo-controlled, masked assignment trials[19][20] Short forms appear to retain sensitivity to treatment effects while substantially reducing burden[20][21] |
| Clinical utility | Good | Free (public domain), strong psychometrics, extensive research base. Biggest concerns are length and reading level. Short forms have less research, but are appealing based on reduced burden and promising data |
Interpretation
GBI Scoring
The current GBI questionnaire includes 73 Likert-type items which reflect symptoms of different moods. The original version of the GBI used case scoring where items were given values ranging from 1-4. Symptoms that were rated as 1 or 2 were considered to be absent and symptoms rated as 3 or 4 were considered to be present. However, if each item were to receive one of four scores, the authors of the GBI decided Likert scaling would be a better scoring option. The items on the GBI are now scaled from 0-3 rated as 0 (never or hardly ever present), 1 (sometimes present), 2 (often present), and 3 (very often or almost constantly present).[14]
PGBI-10M
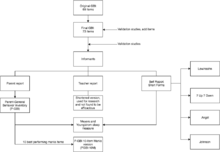
For the PGBI-10M, the scores from each question are added together to form a total score, with higher scores indicating a greater severity of symptoms. Scores range from 0 to 30. Low scores of 5 and below indicate a very low risk of a bipolar diagnosis. High scores of 18 and over indicate a high risk of a diagnosis of bipolar disorder, increasing the likelihood by a factor of seven or greater.[22][23] Several peer-reviewed research studies support the P-GBI as a reliable and valid measure of bipolar in children and adolescents.[23][24] It is recommended to be used as part of an assessment battery in the diagnosis of juvenile bipolar disorder.
Adverse effects
Being a self-report questionnaire, the GBI is not known to have any adverse effects on patients beyond the potential of causing minor distress.
Mechanism
The GBI takes about 10 to 30 minutes to complete, and it has a 12th grade reading level .
Research
Shorter versions of the GBI have been validated for research and clinical use. For instance, the PGBI-10M is currently being tested as part of a large longitudinal study investigating the course of early symptoms of mania in children , with preliminary studies indicating its clinical efficacy in differentiating juvenile bipolar disorder from youth with other diagnoses .
See also
- Diagnostic classification and rating scales used in psychiatry
- Rating scales for depression
- Bipolar disorder
References
- ↑ Dr. Richard Depue
- ↑ Youngstrom, Findling, Danielson; et al. (2001). "Discriminative validity of parent report of hypomanic and depressive symptoms on the General Behavior Inventory". Psychol Assess.
- 1 2 3 Youngstrom, Frazier, Demeter, Calabrese, & Findling (2008). "Developing a Ten Item Mania Scale from the Parent General Behavior Inventory for Children and Adolescents". J Clin Psychiatry.
- 1 2 Youngstrom, Eric A.; Murray, Greg; Johnson, Sheri L.; Findling, Robert L. (2016-12-01). "The 7 Up 7 Down Inventory: A 14-item measure of manic and depressive tendencies carved from the General Behavior Inventory". Psychological assessment. 25 (4): 1377–1383. doi:10.1037/a0033975. ISSN 1040-3590. PMC 3970320
 . PMID 23914960.
. PMID 23914960. - ↑ Achenbach, TM; McConaughy, SH; Howell, CT (March 1987). "Child/adolescent behavioral and emotional problems: implications of cross-informant correlations for situational specificity.". Psychological Bulletin. 101 (2): 213–32. PMID 3562706.
- 1 2 3 4 5 Depue, Richard A.; Slater, Judith F.; Wolfstetter-Kausch, Heidi; Klein, Daniel; Goplerud, Eric; Farr, David (1981). "A behavioral paradigm for identifying persons at risk for bipolar depressive disorder: A conceptual framework and five validation studies.". Journal of Abnormal Psychology. 90 (5): 381–437. doi:10.1037/0021-843X.90.5.381.
- ↑ Klein, DN; Dickstein, S; Taylor, EB; Harding, K (February 1989). "Identifying chronic affective disorders in outpatients: validation of the General Behavior Inventory.". Journal of consulting and clinical psychology. 57 (1): 106–11. PMID 2925959.
- ↑ Mesman, Esther; Nolen, Willem A.; Reichart, Catrien G.; Wals, Marjolein; Hillegers, Manon H.J. (May 2013). "The Dutch Bipolar Offspring Study: 12-Year Follow-Up". American Journal of Psychiatry. 170 (5): 542–549. doi:10.1176/appi.ajp.2012.12030401.
- ↑ Reichart, CG; van der Ende, J; Wals, M; Hillegers, MH; Nolen, WA; Ormel, J; Verhulst, FC (December 2005). "The use of the GBI as predictor of bipolar disorder in a population of adolescent offspring of parents with a bipolar disorder.". Journal of affective disorders. 89 (1-3): 147–55. PMID 16260043.
- ↑ Depue, RA; Kleiman, RM; Davis, P; Hutchinson, M; Krauss, SP (February 1985). "The behavioral high-risk paradigm and bipolar affective disorder, VIII: Serum free cortisol in nonpatient cyclothymic subjects selected by the General Behavior Inventory.". The American journal of psychiatry. 142 (2): 175–81. PMID 3970242.
- ↑ Klein, DN; Depue, RA (August 1984). "Continued impairment in persons at risk for bipolar affective disorder: results of a 19-month follow-up study.". Journal of abnormal psychology. 93 (3): 345–7. PMID 6470321.
- 1 2 Pendergast, Laura L.; Youngstrom, Eric A.; Brown, Christopher; Jensen, Dane; Abramson, Lyn Y.; Alloy, Lauren B. (2015). "Structural invariance of General Behavior Inventory (GBI) scores in Black and White young adults.". Psychological Assessment. 27 (1): 21–30. doi:10.1037/pas0000020.
- 1 2 Danielson, CK; Youngstrom, EA; Findling, RL; Calabrese, JR (February 2003). "Discriminative validity of the general behavior inventory using youth report.". Journal of abnormal child psychology. 31 (1): 29–39. PMID 12597697.
- 1 2 Findling, RL; Youngstrom, EA; Danielson, CK; DelPorto-Bedoya, D; Papish-David, R; Townsend, L; Calabrese, JR (February 2002). "Clinical decision-making using the General Behavior Inventory in juvenile bipolarity.". Bipolar disorders. 4 (1): 34–42. PMID 12047493.
- ↑ Youngstrom, Eric A.; Genzlinger, Jacquelynne E.; Egerton, Gregory A.; Van Meter, Anna R. (2015). "Multivariate meta-analysis of the discriminative validity of caregiver, youth, and teacher rating scales for pediatric bipolar disorder: Mother knows best about mania.". Archives of Scientific Psychology. 3 (1): 112–137. doi:10.1037/arc0000024.
- ↑ Alloy, LB; Abramson, LY; Hogan, ME; Whitehouse, WG; Rose, DT; Robinson, MS; Kim, RS; Lapkin, JB (August 2000). "The Temple-Wisconsin Cognitive Vulnerability to Depression Project: lifetime history of axis I psychopathology in individuals at high and low cognitive risk for depression.". Journal of abnormal psychology. 109 (3): 403–18. PMID 11016110.
- ↑ Klein, Daniel N.; Dickstein, Susan; Taylor, Ellen B.; Harding, Kathryn (1989). "Identifying chronic affective disorders in outpatients: Validation of the General Behavior Inventory.". Journal of Consulting and Clinical Psychology. 57 (1): 106–111. doi:10.1037/0022-006X.57.1.106.
- ↑ Youngstrom, EA; Findling, RL; Danielson, CK; Calabrese, JR (June 2001). "Discriminative validity of parent report of hypomanic and depressive symptoms on the General Behavior Inventory.". Psychological assessment. 13 (2): 267–76. PMID 11433802.
- ↑ Findling, RL; Youngstrom, EA; McNamara, NK; Stansbrey, RJ; Wynbrandt, JL; Adegbite, C; Rowles, BM; Demeter, CA; Frazier, TW; Calabrese, JR (January 2012). "Double-blind, randomized, placebo-controlled long-term maintenance study of aripiprazole in children with bipolar disorder.". The Journal of clinical psychiatry. 73 (1): 57–63. PMID 22152402.
- 1 2 Youngstrom, E; Zhao, J; Mankoski, R; Forbes, RA; Marcus, RM; Carson, W; McQuade, R; Findling, RL (March 2013). "Clinical significance of treatment effects with aripiprazole versus placebo in a study of manic or mixed episodes associated with pediatric bipolar I disorder.". Journal of child and adolescent psychopharmacology. 23 (2): 72–9. PMID 23480324.
- ↑ Ong, ML; Youngstrom, EA; Chua, JJ; Halverson, TF; Horwitz, SM; Storfer-Isser, A; Frazier, TW; Fristad, MA; Arnold, LE; Phillips, ML; Birmaher, B; Kowatch, RA; Findling, RL; LAMS, Group (1 July 2016). "Comparing the CASI-4R and the PGBI-10 M for Differentiating Bipolar Spectrum Disorders from Other Outpatient Diagnoses in Youth.". Journal of abnormal child psychology. PMID 27364346.
- ↑ "Table of all screening tools and rating scales". Massachusetts General Hospital: School Psychiatry Program and MADI Resource Center. Massachusetts General Hospital. Retrieved 22 September 2015.
- 1 2 Youngstrom, EA; Frazier, TW; Demeter, C; Calabrese, JR; Findling, RL (May 2008). "Developing a 10-item mania scale from the Parent General Behavior Inventory for children and adolescents.". The Journal of Clinical Psychiatry. 69 (5): 831–9. doi:10.4088/jcp.v69n0517. PMID 18452343.
- ↑ Youngstrom, E; Meyers, O; Demeter, C; Youngstrom, J; Morello, L; Piiparinen, R; Feeny, N; Calabrese, JR; Findling, RL (December 2005). "Comparing diagnostic checklists for pediatric bipolar disorder in academic and community mental health settings.". Bipolar disorders. 7 (6): 507–17. doi:10.1111/j.1399-5618.2005.00269.x. PMID 16403176.